หมวดหมู่ของบทความนี้จะพูดถึงc-spine คือ หากคุณกำลังมองหาc-spine คือมาถอดรหัสหัวข้อc-spine คือกับbirthyouinlove.comในโพสต์Cervical Spine Trauma – Everything You Need To Know – Dr. Nabil Ebraheimนี้.
สารบัญ
ข้อมูลทั่วไปเกี่ยวกับc-spine คือในCervical Spine Trauma – Everything You Need To Know – Dr. Nabil Ebraheimที่สมบูรณ์ที่สุด
ที่เว็บไซต์BirthYouInLoveคุณสามารถเพิ่มเอกสารอื่น ๆ นอกเหนือจากc-spine คือสำหรับข้อมูลที่เป็นประโยชน์มากขึ้นสำหรับคุณ ที่เว็บไซต์BirthYouInLove เราอัปเดตข้อมูลใหม่ ๆ ที่ถูกต้องให้คุณทุกวัน, ด้วยความหวังว่าจะได้บริการที่คุ้มค่าที่สุดแก่ผู้ใช้ ช่วยให้คุณเพิ่มข้อมูลออนไลน์ได้อย่างรวดเร็ว.
คำอธิบายบางส่วนที่เกี่ยวข้องกับหมวดหมู่c-spine คือ
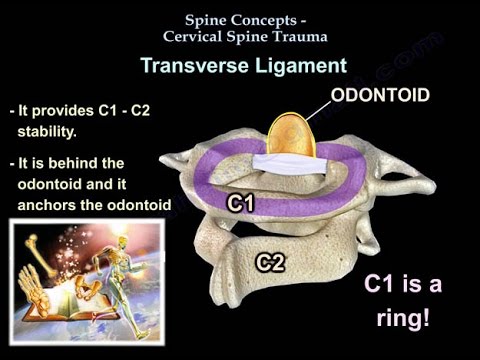
ภาพเคลื่อนไหวเพื่อการศึกษาของ Dr. Ebraheim แสดงให้เห็นแนวคิดเกี่ยวกับกระดูกสันหลังที่เกี่ยวข้องกับกระดูกสันหลังส่วนคอ – การบาดเจ็บ เอ็นตามขวาง: – ช่วยให้ C1-C2 มีความมั่นคง – อยู่ด้านหลังฟันและยึดฟันกับวงแหวน C1 เพื่อป้องกันการเคลื่อนไหวผิดปกติระหว่าง C1 และ C2 – ADI ในผู้ใหญ่ 3.5 มม. – จากอาการบาดเจ็บที่เอ็นตามขวาง C1 และ C2 จะเคลื่อนไหวได้อย่างอิสระและจะมี ADI เพิ่มขึ้น – การบาดเจ็บที่เอ็นตามขวางที่แยกออกมาอาจหาได้ยาก – เจฟเฟอร์สันหัก สามประเภท: – ประเภท II: แตกหักที่ฐานของกระบวนการจัดฟัน ส่วนใหญ่แตกหักยาก – อัตรา Nonunion อยู่ที่ 20-80% เนื่องจากการหยุดชะงักของปริมาณเลือด – อัตรา nonunion สูงใน: – มากกว่า 5 มม. displacement. – ผู้ป่วยอายุมากกว่า 50 ปี – ปัจจัยเสี่ยงอื่น ๆ : – การรักษาล่าช้า – กระดูกหักหลังเคลื่อน – โรคเบาหวาน – ห้ามใช้รัศมีในผู้ป่วยระยะแรก เสี่ยงต่อการเสียชีวิตจากโรคปอดบวม – การรักษาผู้ป่วยเด็ก: • รัศมี: อาจต้องใช้แรงฉุดรัศมีในขั้นต้นเพื่อลดการแตกหัก รัศมีนานถึง 3 เดือน อัตรา 30% ที่ไม่ใช่สหภาพในรัศมี • คุณทำศัลยกรรมเมื่อไหร่? การแตกหักในผู้ป่วยสูงอายุ ปัจจัยเสี่ยงของการไม่มีสหภาพแรงงาน • นิยมใช้สกรูจัดฟันในผู้ป่วยเด็ก • ต้องรักษาการเคลื่อนที่ของ C1-C2 • ห้ามทำฟิวชันในผู้ป่วยเด็ก • สามารถใช้ C1-C2 fusion ในผู้ป่วยสูงอายุได้ • สำหรับผู้ป่วยสูงอายุ: – Orthosis หรือ Fusion of C1- C2 หากมีข้อบ่งชี้สำหรับการผ่าตัดและหากมีการอนุมัติสำหรับการผ่าตัด Type III: – การแตกหักผ่านร่างกายของ C2 – การรักษา: • orthosis ของปากมดลูก • Halo: ถ้าเคลื่อนย้าย • การแตกหักของเพชฌฆาตเป็นการแตกหักแบบทวิภาคีของ pars interarticularis • คลองไขสันหลังกว้างขึ้นและจะมีความเสี่ยงต่ำต่อการบาดเจ็บไขสันหลัง การจำแนกประเภท Levine และ Edwards: – Type I: การแตกหักที่มั่นคงโดยมีการกระจัดน้อยกว่า 3 มม. ไม่มีการโค้งงอ การรักษา: orthosis ของปากมดลูก – ประเภท II: ประเภทที่พบบ่อยที่สุด, การแปลที่สำคัญและมุมบางส่วน, การแตกหักที่ไม่เสถียร, การรักษา: การดึงปากมดลูกและการยืดออกเพื่อปรับปรุงการเคลื่อนย้าย, การตรึงในรัศมีเสื้อกั๊กประมาณ 3 เดือน – ประเภท IIa: การโค้งงออย่างรุนแรงและการแปลเล็กน้อยในการบาดเจ็บจากการงองอด้วยการฉีกขาดของเอ็นตามยาวหลัง การแตกหักไม่เสถียร การรักษา: ห้ามใช้แรงดึงเมื่อมีมุมหักอย่างรุนแรง – Type III: ประเภทการผ่าตัด, C2-C3 facet dislocation, การแตกหักของ pedicles ที่หายากนอกเหนือจากความคลาดเคลื่อนด้านหน้า, มีการเชื่อมโยงการขาดดุลทางระบบประสาท, การรักษา: การผ่าตัดเพื่อลดความคลาดเคลื่อนด้านและการรักษาเสถียรภาพของการบาดเจ็บ, การลดแบบเปิด . และการรวมกระดูกสันหลังส่วนหลัง ความคลาดเคลื่อนด้าน: ความสัมพันธ์ของหมอนรองกระดูกเคลื่อนและการมีส่วนร่วมของด้านนั้นสูงมาก ดังนั้นให้ระวังหมอนรองกระดูกเคลื่อนนอกเหนือจากการบาดเจ็บของกระดูก – ความคลาดเคลื่อนด้านเดียวมักจะมีการแปลเอ็กซ์เรย์น้อยกว่า 50% และอาจส่งผลต่อรากประสาท – ความคลาดเคลื่อนด้านทวิภาคีจะมีการแปลมากกว่า 50% และอาจเป็นอาการบาดเจ็บที่ไขสันหลัง – การรักษา: การลดขนาดปิดทันที รับ MRI จากนั้นทำการผ่าตัด หากผู้ป่วยมีอาการทางจิตเปลี่ยนแปลง ให้ทำ MRI ก่อน แล้วตามด้วยการผ่าตัดลดขนาดเปิดและการผ่าตัดตรึงทันที – คุณจะไปข้างหน้าเมื่อไหร่? – ไปข้างหน้าหากมีหมอนรองกระดูกเคลื่อน อุบัติการณ์ประมาณ 10%-30% ในการเคลื่อนด้านของปากมดลูก – หากคุณพยายามลดขนาด แผ่นดิสก์อาจค้างอยู่ในคลอง ทำให้เกิดอาการบาดเจ็บที่ไขสันหลังได้ – เมื่อไหร่ที่คุณทำหลัง? – หากความคลาดเคลื่อนล้มเหลวและไม่มีแผลพุพอง – เมื่อไหร่ที่คุณรวมขั้นตอนด้านหน้าและด้านหลัง? – ต้องไปข้างหน้าเพื่อเอาแผ่นดิสก์ออก – ต้องไปทางด้านหลังเนื่องจากความคลาดเคลื่อนไม่สามารถลดลงได้โดยวิธีปิดหรือโดยเทคนิคเปิดด้านหน้า • จุดสำคัญ: 1- รับ MRI ก่อนการผ่าตัด: ตรวจสอบให้แน่ใจว่าไม่มีหมอนรองกระดูกเคลื่อน 2- อาการบาดเจ็บเอ็นไม่หาย ต้องผ่าตัดฟิวชัน 3- รู้การจัดเรียงของด้าน: ด้านที่เหนือกว่าและด้านที่ด้อยกว่าในตำแหน่งปกติ, ซับลักซ์, และเคล็ด รู้จัก “ด้านเปล่า” หรือ “ด้านที่ว่างเปล่า” ฝึกฝนตัวเองให้รู้สิ่งนี้ โดยเฉพาะอย่างยิ่งสำหรับคำถามในการสอบ หน้าเปลือย. กระดูกสันหลังส่วนคอ MRI Facet Fracture การบาดเจ็บที่เอ็นของกระดูกสันหลังส่วนคอ Burst Fracture of Lower Cervical Spine Tear Drop Fracture ติดตามฉันบน Twitter: บริจาคให้กับมูลนิธิ University of Toledo แผนกศัลยกรรมกระดูกและข้อบริจาคกองทุนเก้าอี้: .
รูปภาพที่เกี่ยวข้องกับหมวดหมู่ของc-spine คือ
นอกจากการหาข่าวเกี่ยวกับบทความนี้แล้ว Cervical Spine Trauma – Everything You Need To Know – Dr. Nabil Ebraheim คุณสามารถค้นพบเนื้อหาเพิ่มเติมด้านล่าง
เนื้อหาเกี่ยวกับc-spine คือ
#Cervical #Spine #Trauma #Nabil #Ebraheim.
cervical spine,rheumatoid arthritis,total hip arthroplasty,myelopathy,subaxial subluxation,transverse ligament,odontoid,champerlain’s line,foramen magnum,skull,C1,C2,laxity,tear,osteophyte formation,vertebra,MRI,XRAYS,Dr. Nabil Ebraheim,Nathan Elkins,UTMC,orthopaedics,UT,miranda,lumbar disc,radiculopathy.
Cervical Spine Trauma – Everything You Need To Know – Dr. Nabil Ebraheim.
c-spine คือ.
เราหวังว่าค่านิยมบางอย่างที่เรามอบให้จะเป็นประโยชน์กับคุณ ขอขอบคุณที่อ่านบทความของเราเกี่ยวกับc-spine คือ
I've been watching Dr.Ebraheims videos for about a month now trying to learn more about my sons unfused dens. Over a year ago we rushed him to the emergency room at a local hospital & after physical evaluation & xrays the emergency physician recommended that we take him to UC Davis here in sacramento ca. for a CAT SCAN & MRI due to his finding the unfused dens on xray.
After 24 hours spent in a hospital room we were introduced to 12 physicians from the UC Davis spinal center. We were told that nothing was hurt or injured & his physical test came out great. I then asked what about his unfused dens? and the lead physician said that it was just imaging that a lot of people have it yet go on with a normal life.The only thing they wanted us to do was refrain our son from any contact sport for 2 weeks than he may start back as he feels. My son plays youth football & does well at it but my wife wanted a 2nd opinion so she took him to shriners than a 3rd opinion from Stanford sports medicine & both Shriners & Stanford agreed that he can no longer play football due to his unfused dens even though the rest of his team might have unfused dens being that they are all the same age but that is a parents choice i was told. Last month we went for a yearly check up & yes his dens are fusing but still no clearance for any kind of sports activity. Dr.Ebraheim you are a renowned spinal specialist is this really the end for my 9 year old sons future in sports? pls advise my son has not stopped his training which consist of 2 /12 hours of physical training 5 days a week all year since he was told he could not play anymore,But keeps asking when can he play again & its hard for me as a parent that i can not give him an answer.
May I ask would prolotherapy heal a ligament injury and help facet joints? Caring Medical show xray, and digital motion xray results of improvement. It is successfully used for ligament sport injuries, early intervention for degenerative hips etc. However I dont know if it would be possible to reach the ligament at C1/2?
Nabil ibrahim best dr for ever l seen
How cervical affect brain stem
Currently sitting in the hospital. Had a c1 fracture cause of a car accident. I can walk and everything fine and have all my senses. Luckily it wasn't as bad as it could have been
Great teacher
Are you aware of prolotherapy to heal ligaments?
Great video! Thank you.
Thank you
Thank u so much .
Thanks
कृपया हिंदी मे भी सिखाए
How can halo cause pneumonia ?
Sir,
My cervical spine c2#
Spindle cort is normal.
6 week complete .
But last 4to 5 day left hand and lag mild tingling and numbness .
Sir please suggest me.
Why could elderly patients die from Pnemonia with a halo ?
Hi sir i am from nepal now at in qatar for job …How can i contact you ..my spainal cord c1 C2 fracture…plz reply me plz .
Very simple and good explanation
Fantastic
HEY! PLS answer this question! thank you. So, this morning I woke up and it was very cold, then I went to the toilet to pee. I sat down for awhile and decided to turn my head diagonally to crack it, as soon as I cracked it i heard quite a loud pop on the right back of my neck and it started to hurt. I then felt a bump on the back of my neck, I'm not sure but I think is the c7. I'm scared if it's dislocated or broken. I don't feel any numbness anyone, or pain anywhere else but the back right side of my neck . Can you help me diagnose my situation. today is the second day after this incident.
Speech and swalling problem for this ?
thank you for your effort
very helpful
V useful videos ….
Telugu lo
Very informative,concise excellent vedios
Please doctor Ebraheim how can one see you ? I am having neurological symptoms and I have been to many doctors with no answers. How can you help me ? Please I need your help
Thanks for nice helpful video
What about facet joint pain in cervical C1 C2? There is a lot of arthritis. Why do facet joints hurt there? Are there nerves inside the cervical facet joint?
THANK YOU SIR ANOTHER AMAZING VIDEO
Dr. Ebraheim you are a GODSEND, thank you for your video!
Need a video on Alar and Accessory ligaments for C1/C2
Best Cervical Video ever!
God bless you Sir
I have a ruptured disc in my C-spine that happened from a car accident going on 9yrs now. I never got surgery for it. I just had a new MRI of my neck to keep an eye on it and it shows spinal cord compression with fractures in the vertebra ..i am thinking probably compression fractures for not having injury on my neck for so long and my body trying to compensate for the injury. do you have an email where I can send you a picture of the MRI to see if it is an emergency situation. I am afraid if I leave it, that I will end up in a wheel chair. I as well have a ruptured disc in my lower lumbar spine as well, with early DDD and loss of T2, hyperintensity at L3-4 L 4-5- L5-S1. with encroachment on the descending left L5 nerve. foraminal stenosis with encroachment on the exiting L4 nerve. spinal stenosis, and advanced facet arthropathy. central protrusion with annular tear, foraminal stenosis. list goes on. thank you….
Thank you for your video. You do a great job!
I want to add that C1-2 can become unstable with connective tissue disorders such as Ehlers Danlos Syndrome without any trauma or with trauma due to faulty ligaments because of the connective tissue disorder. CT scan with 90•rotation shows this as most often static imaging doesn’t show how unstable it truly is. I walked around for 3 years disabled and felt like I was dying with many neurological symptoms. I had 10mm to the left and 8mm right translation because static imaging did not show this. I was dismissed for 3 years because of static imaging!! It’s so important to to add that rotation into the imaging. I’m lucky to be alive today because I didn’t give up searching for answers.
اعانكم الله شكرا#الجزائر
Another brilliant video. Informative and interesting
I love your videos! Just one minor (audio) mistake at 6:53 you said "pedicle" of C2 but have it written correctly as pars interarticularis. Great video nonetheless! Keep them coming